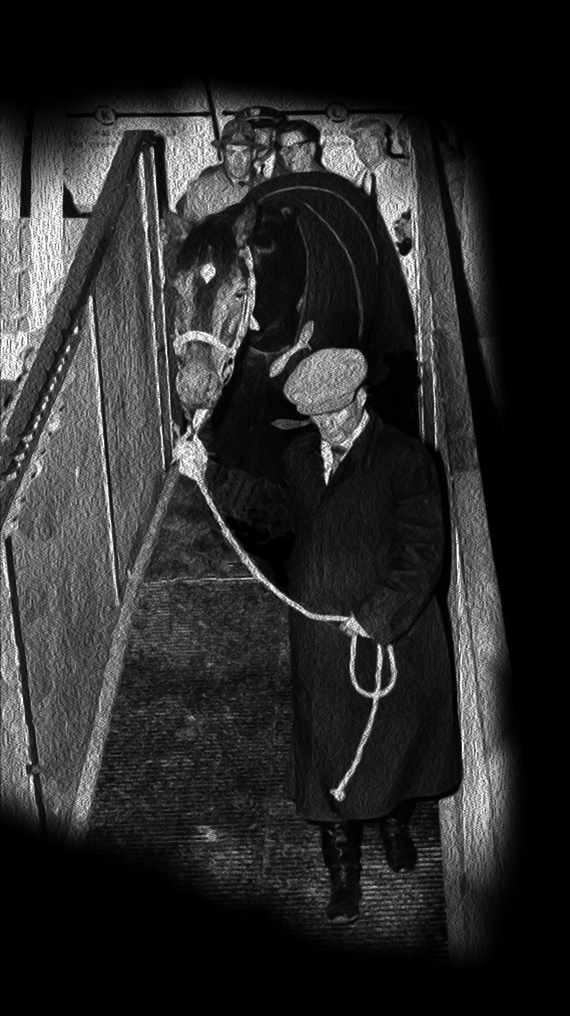
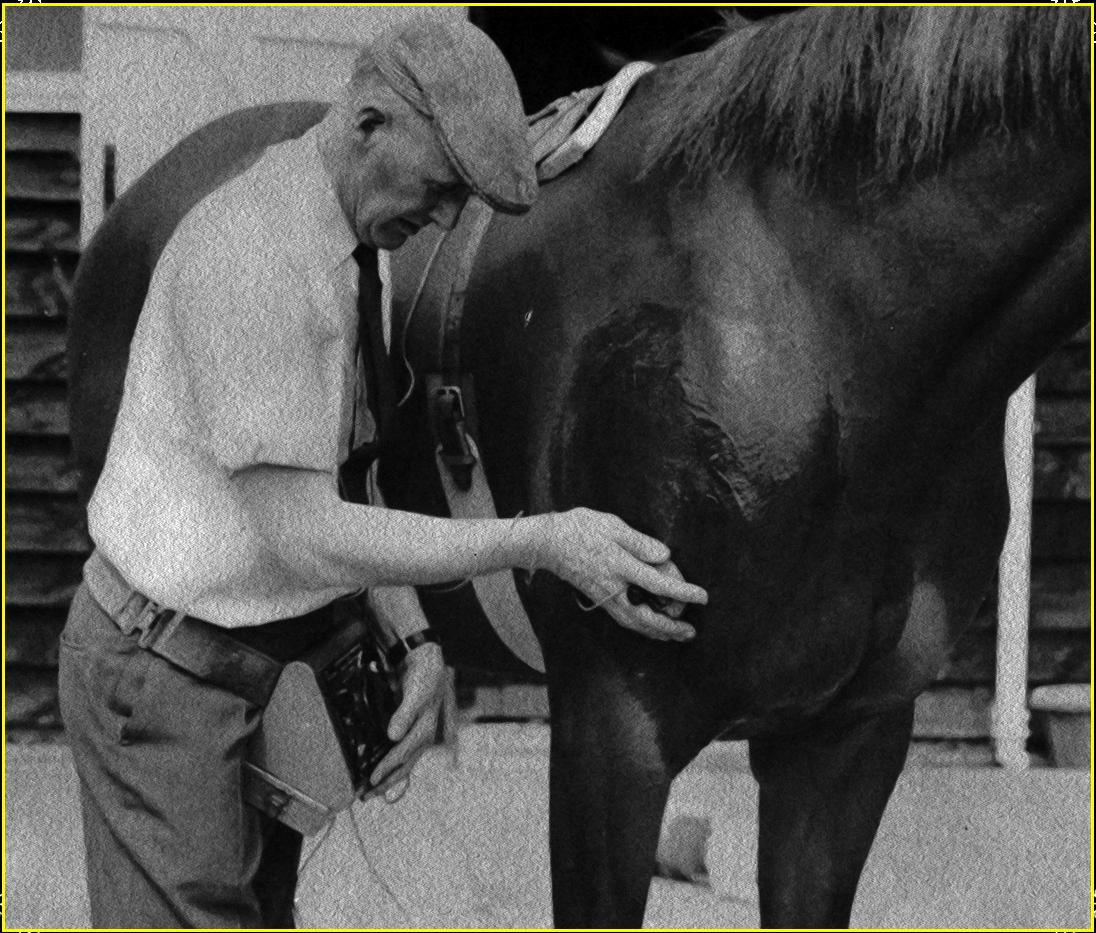
Above is the photo of my mentor of the 1970's when I was a college boy with hopes of training the best racehorses possible. He is shown applying a positive electrode to the shoulder of a horse to artificially contract those muscle fibers. He is the Brit, Charles L. Strong, who authored the book, Horse Injuries, Common-Sense Therapy of Muscles and Joints for the Layman (1973, Arco). I devoured that book as a young man and carried it with me to every racetrack, I ever trained and raced. It taught me much, but probably the most crucial lesson was that injury often produces adhesions at the damaged site which needs to be broken up whether by actual on-track exercise or artificially by electronic muscle stimulation. Since injured horses are seldom judiciously exercised, an artificial means of stimulating selective muscle movement proved a superb answer to improved healing! His book taught me how important muscle contractions were in healing tissue damage by stimulating blood & lymph circulation, increasing cellular metabolism, and pointing the way for the strongest regeneration of damaged tissue. It stressed how important muscle movement was in the painless ranges immediately following a new injury when most vets would say to utilize complete rest and apply cold -- opening up the injury to adhesion formation and atrophy. Leg paints, blisters, hot whirlpool baths, etc may all be beneficial in improving blood supply, but none can equal the superiority of actual muscle movement, exercise in the injured racehorse which not only pulls blood and lymph in but pumps it out, too! This is a premise that should never be forgotten by any racehorse trainer!
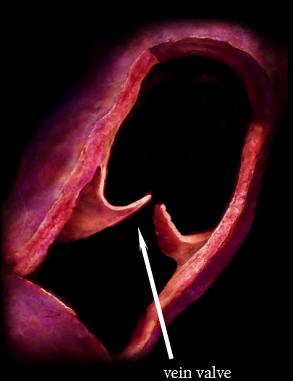
Movement is the best and most natural action to keep tissue fed with fresh arterial oxygen-rich, nutritious blood while at the same time pumping the toxic by-products of cell metabolism and injury out via the veins and lymphatics. Arteries do not have inner one-way valves, but veins and the lymphatic system does. If you force rest the muscles and tissue designed to function in movement; you can risk decreased healing. Muscular activity is particularly important in venous and lymphatic circulations, since they work best in coordination with body movement. Movement produces a pumping action in both of these systems keeping their fluids moving forward with the help of the one-way valves as seen to the right. It is quite common to see stalled horses "stock-up" (swell) in the lower legs overnight. This is a stagnation of fluids derived from non-movement and commonly observed after extended stall rest in the mornings. I always marveled at the clean definition of my horses' legs after a long ship in a bouncy rough-riding van. They all walked down the ramp with their legs in pristine condition which shows the power of leg movement, even if they are just standing in one place!
When injury occurs, a number of things happen:
1) escape of blood into the surrounding tissue,
2) lymph seeping from damaged lymphatic vessels which can cause adhesion formation,
3) blood congestion which can cause chronic future structural problems if left too long,
4) a localized anemia due to obstructions in the injured area,
5) muscle atrophy,
6) muscle hypertrophy due to stimulated connective tissue formation,
7) increased inflammation beyond what is needed for actual tissue repair,
8) formation of non-elastic scar, adhesive tissue not only at site of injury but into surrounding tissues.
The latter is probably the most insidious of what may cause lasting damage to a racehorse's performance--ADHESIONS! Adhesion formation must be addressed by the trainer soon after injury! When damage occurs, the various above mentioned fluids seep into the injured site and surrounding area to stabilize the damage. It is nature's way. This is all well and good in the very beginning, but if motion is limited these adhesions can be maintained and result in not only the injured site becoming inelastic but some of the surrounding area as well, limiting movement range even further. Adhesions are most likely to occur in tendon sheaths (commonly seen in bowed tendons), in ligaments such as the suspensory, joint linings, and muscle bundles. Pain is a natural component of adhesions. This lingering pain from a lingering adhesion can often be wrongly diagnosed by the trainer and his connections as simply a "loss of form" in a horse that seems otherwise sound on the track. Big mistake! The use of electronic muscle stimulation can help prevent such formations.
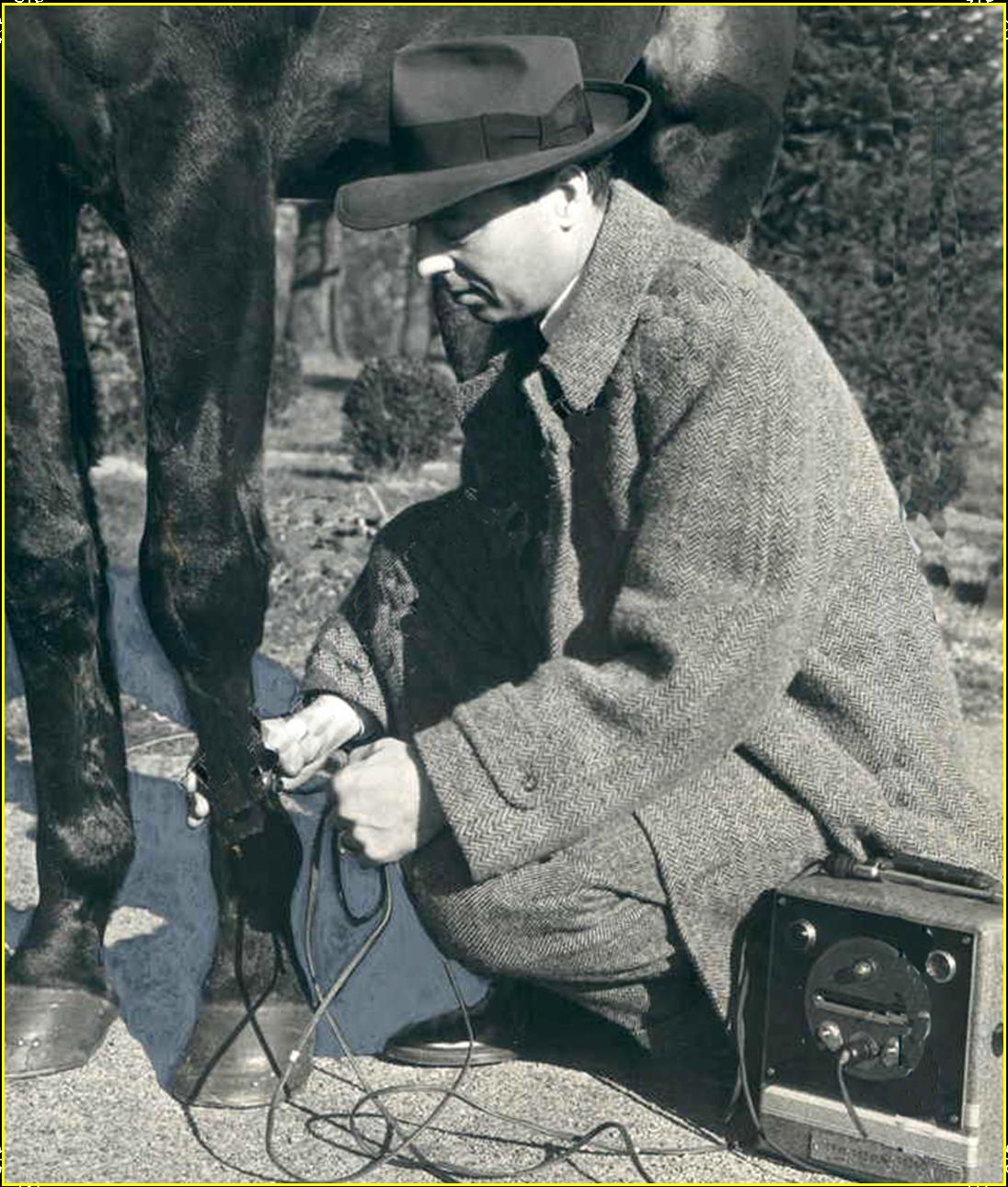
Charles Strong probably could be considered the father of equine electro-mediicne. His instrumentation looks primitive by today's standards, but he was the first to point the way and his truths for injury repair are just as relevant today as back then. In 1939, Lord Mountbatten asked him to apply his protocol to some injured polo ponies after he treated injured polo players on Mountbatten's team with remarkable success. Accordingly, Charles Strong tried his method on the ponies and the use of therapeutic electronic muscle contractions in the equine was born! Strong was using a waveform known as "Faradic" which is interrupted direct current with pulse duration 0.1 - 1 ms and frequency in between 50 - 100 Hz. Faradic current stimulates the motor nerve in the muscle bundle to contract mimicking the movement in the patient. It then, surges, causing a relaxation. Hence, Strong called his waveform, Rhythmic Muscular Contractions. I mentioned Faradic in Part 1 as one of the first waveforms commonly used in medicine at the turn of the 20th century. It has been around a long time There are now better, more efficient therapeutic waveforms out there than Faradism. The Russian mode of electrical muscle stimulation developed in the 1970's is generally considered to be superior. It was found that the higher frequency of 2500 Hz which the Russian mode uses was far more comfortable for the patient than lower frequencies such as the 50-100 Hz used by Faradism. It was also discovered that greater current could be delivered more comfortably at these higher frequencies producing more work and improved muscular contractions.
Electrical Muscle Stimulation (EMS)
EMS or electrical muscle stimulation is best performed using the so called Russian Mode which most EMS machines will generate. Another name for the Russian mode is Burst Mode Alternating Current (BMAC). Its frequency is 2500 Hz delivered in a pulsed output. 2500 Hz is the most comfortable frequency to use along with the pulsed output to get maximum muscle stimulation with the least discomfort and power generation. This wave form was developed by the Russians for their Olympic athletes. It is considered one of the most therapeutic form to electrically contract & relax the major muscle groups. This is the mode that one should use when treating equine suspensory and tendon injuries and may be of use in rear-end muscle injuries as well. The traditional stimulation protocol is known as 10 / 50 / 10 or in other words, 10 seconds of stimulation, 50 seconds of rest, all done in a 10 minute session. This is for each muscle bundle. If one tries to stimulate for longer than 10 seconds at maximum intensity, fatigue sets in. Daily use is recommended.
Lastly, an interesting study done in 2009 comparing Russian to TENS found that there was no discernable difference in the two when pain relief is being treated. In fact, it was found that the Russian wave form was more comfortably tolerated by the patient than TENS.
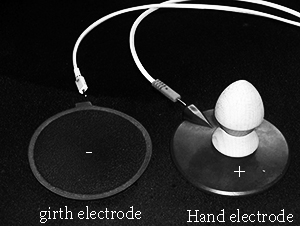
I would also like to discuss the EMS unit, itself, which I did to some extent also on the suspensory injury page. It would be nice if we had cheap access to an EMS unit like Charles Strong's Transeva machine for veterinary applications. Most of us don't. First off, they are hard to obtain and secondly, they are outrageously expensive. There is no reason why a human EMS machine like the ones used in many clinics and offices cannot be re-tooled to use on the equine. They can be had cheaply and they produce exactly the type of wave we need. The older analog models that are being upgraded and are out there for sale have knobs which are more desirable for veterinary use, too. The only problems are the electrodes and applying the electrodes to a hairy coat which humans do not have. Charles Strong worked around this problem by thoroughly saturating the hair coat with a conductive gel or salt water. He placed his negative electrode as a stationary electrode directly over the withers area with the help of an electrode "saddle" held in place by an elastic girth. He then used the positively charged electrode as a mobile device which he placed in his hand directly over the muscle bundles he wished to stimulate, keeping it stationary for treatment and then moving it as he saw fit to the next appropriate muscle bundle. His free hand could manipulate amplitude at the same time. We can simulate this with a human device in one of two ways. We can like him, use the negative electrode as a stationary structure over the withers held in place by an elastic girth. That is easy enough to do. Also, like him, we can then take with our free hand the positive electrode and move it over the muscle bundles being treated. This can be accomplished by modifying a human EMS configuration and electrodes. You will need some heavy-duty, rubber/carbon 4" electrodes which should cost around US$10-15 each. They are not that common, but can be found on the Internet if you search hard. These heavy-duty electrodes can then be modified to simulate the Charles Strong configuration. One can add a wood or plastic knob to one electrode which will be the mobile positive one held in the hand. The other electrode will be negatively charged and attach to a makeshift saddle and elastic girth over the withers region. A knob can be easily found and simply screw it from the underside of he electrode into the knob for an easy movable electrode as seen to the right.
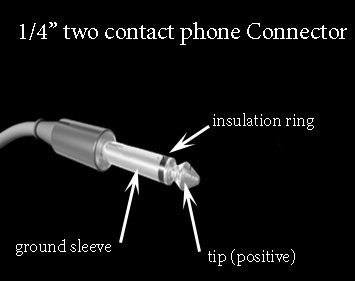
The electrodes leads will be the next problem to solve when duplicating the Charles Strong configuration on a human unit. We will need to have a very long set of leads that will reach to the top of the withers to the negative electrode and at the same time its companion lead will go to the practitioner's hand holding the mobile positive electrode that will be moving around the horse. Most human leads will not be long enough. There is nothing really magical about finding appropriate lead wires and applying them to our electrodes. Depending on your EMS unit you will have to find an appropriate plug-in and then attach wires to it, terminating in a 2 mm pin which most electrodes use for connection purposes. I tend to prefer the Rich-Mar brand of EMS machines as they are well built by a global company. There is also plenty of support online in the form of manuals. The Rich-mar units tend to use a 1/4" or 6.35 mm, two-contact audio phone type of connector. One simply has to find a cable that will accommodate this type of plug and configure cables that will end with a 2 mm pin connection for the electrodes. I have found that musical instrument type cables work quite well on the Rich-mar units. They are much cheaper to buy than if you went to the company for their specialized cables. If you are using a different brand of EMS machine, you will have to find out what type of plug-ins are required and go from there to wire up long enough leads for equine work. You may just want to try to find long 10 foot generic leads and some chiropractor supply houses can sell you them. Split the 10' lead into separate negative and postive cables and that will give you an approximate 15' area to work with for both leads. That should allow you plenty of room for a horse. Check out www.chirocity.com for leads that may fit your particular machine.